Comments:
A healthy 48 year old male presented with atypical chest pain. The discomfort was described as located in the center of the chest that occasionally would awaken him in the middle of the night. He has attributed this in the past to work related stress. He denies any change in exercise tolerance as he runs and bicycles without any difficulty. He has a history of hyperlipidemia with an LDL-C of 205 mg/dl and triglycerides of 195 mg/dl. He had undergone a coronary calcium score with EBCT four years ago demonstrating a score of zero. He did not comply with the recommended prescription of a statin and baby aspirin. His other coronary risk factor was a family history as his father underwent coronary artery bypass surgery at the age of 68.
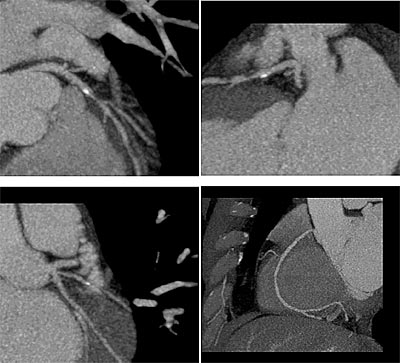
A 64-slice CT Coronary Angiogram at Westside Medical Imaging (WMI) demonstrated an 80% proximal noncalcified plaque in the Left Anterior Descending (LAD) artery. There was mild stenosis in the RCA. His coronary calcium score was only 11. Subsequently a stress test demonstrated left anterior wall ischemia. An invasive coronary angiogram confirmed the severe LAD lesion and he underwent successful revascularization with a coronary stent.
This case report exemplifies the limitations of coronary calcium scoring particularly in young patients. Clinical studies from our large series of patients studied at WMI indicate that the presence of any calcium score >0 greatly increases the risk of significant obstructive disease. |